
TEAM Katie
When Katie Groover volunteered to be in a clinical trial, a team of doctors, nurses and researchers stood behind her every step of the way.

Patients celebrate life beyond a cancer diagnosis 14 . A freezer full of clues 24
WINSHIP BY THE NUMBERS
The mission of Winship Cancer Institute of Emory University is to reduce the burden of cancer by aligning our research with our outstanding patient care. As Georgia’s only National Cancer Institute-designated cancer center, Winship is a national leader in seeking out new ways to defeat cancer and in translating that knowledge into patient care.
• 1979: FIRST BONE MARROW TRANSPLANT AT EMORY.
• 1985: IN ADDITION TO EMORY UNIV. HOSPITAL, WINSHIP BEGINS COORDINATING CANCER RESEARCH AND CARE AT THREE MORE ATLANTA HOSPITALS (CRAWFORD LONG, GRADY, VETERANS AFFAIRS MEDICAL CENTER).
• 2003: WINSHIP OPENS NEW 280,000-SQUAREFOOT, STATE-OF-THE-ART FACILITY.
WINSHIP IS FOUNDED AND ESTABLISHES A CLINIC ON THE EMORY UNIVERSITY CAMPUS; IT TREATS 168 PATIENTS IN ITS FIRST YEAR OF OPERATION.
• 2009: WINSHIP EARNS PRESTIGIOUS CANCER CENTER DESIGNATION BY THE NATIONAL CANCER INSTITUTE.
• GEORGIA’S FIRST AND ONLY NATIONAL CANCER INSTITUTE-DESIGNATED CANCER CENTER.
• IN ADDITION TO PROVIDING CANCER CARE AT THE WINSHIP CANCER INSTITUTE, WINSHIP NOW TREATS PATIENTS AT SEVEN HOSPITALS AROUND THE METRO ATLANTA AREA.

• 14,000 PATIENTS SEEN ANNUALLY.
• 355 CLINICIANS AND RESEARCHERS.
• CURRENTLY CONDUCTING 250 ACTIVE CLINICAL TRIALS.
• 760 PATIENTS ENROLLED IN CLINICAL TRIALS WITHIN THE PAST YEAR.
• 75% OF NEW CANCER TREATMENTS APPROVED BY THE FDA SINCE 2007 HAVE COME THROUGH WINSHIP.
• 436 FUNDED CANCER RESEARCH PROJECTS.
• $28 MILLION IN NCI GRANT FUNDING.
• $87.4 MILLION IN TOTAL GRANT FUNDING.
• 2013: BREAKS GROUND ON EMORY PROTON THERAPY CENTER
Who’s on the cover: Behind every patient is a team of people working to find a cure. Top row from left to right: multiple myeloma project coordinator Kenisha Barron; Phase I nursing tech Keino Friday; senior multiple myeloma researcher Larry Boise; Phase I nurse practitioner Colleen Lewis; researcher Shardule Shah; clinical research nurse Cathy Sharp; oncology nurse practitioner Melanie Watson; multiple myeloma physician/researcher Sagar Lonial. Bottom row left to right: multiple myeloma researcher Yanyan Gu; clinic lab coordinator Fred Johnson; multiple myeloma patient Katie Groover
1940 1950 1960 1980 1970 1990 2000 2010 2020
1937 • 1939
IN THIS ISSUE
Winship in the news 2
Wally Curran celebrates 5th anniversary as executive director; Winship ranks in top 25 cancer programs; 3D mammography now offered.

Stepping up for science
6
Patients who volunteer for clinical trials help advance treatment possibilities for all cancer patients, now and in the future.

Faces of hope
14
From firefighting to tennis, patients and their doctors share what it means to get back into the swing of life.
Every cancer is personal
19
Lung cancers are not all the same. With genomic screening and discoveries in tumor mutations, Winship is developing more precise, individualized treatments.

Finding answers in the freezer
24
A Winship team set out to build a better breast tissue bank for research. Today, that tissue bank is a reality.
Focus on philanthropy
27
Gifts to Winship help support research that advances the fight against cancer.

Editor: Judy Fortin
Managing Editor: Catherine S. Williams
Art Director: Peta Westmaas
Photographer: Jack Kearse
Production Manager: Carol Pinto
Emory | Winship Magazine is published annually by the communications office of the Winship Cancer Institute, a part of the Woodruff Health Sciences Center of Emory University, emoryhealthsciences.org. Articles may be reprinted in full or in part if source is acknowledged. If you have story ideas or feedback, please contact judy.fortin@emory.edu. © Fall 2014. Website: winshipcancer.emory.edu
Emory University is an equal opportunity/equal access/ affirmative action employer fully committed to achieving a diverse workforce and complies with all federal and Georgia state laws, regulations, and executive orders regarding nondiscrimination and affirmative action. Emory University does not discriminate on the basis of race, age, color, religion, national origin or ancestry, gender, disability, veteran status, genetic information, sexual orientation, or gender identity or expression.
6
FALL 2014 19 14
Winship
“The many successful treatments we have for cancer today are here because someone was willing to try a new drug in a trial. Without clinical trials, we would not be able to move medicine forward.”
–R. Donald Harvey, director of the Winship Phase I Clinical Trials Section.
5 Questions for Walter J. Curran, Jr.
This has been an exciting year for Wally Curran. He recently marked his fifth anniversary as executive director of Winship Cancer Institute of Emory University. In June, he became the first Emory physician and Georgia-based doctor to hold a seat on the board of the American Society of Clinical Oncology. Curran ranks among the top 20 researchers nationwide for National Institutes of Health funding.

Q:1
How has Winship Cancer Institute changed since you took the helm in 2009? We’ve seen so many positive changes in the past five years due to the recruitment, retention, and career development of many outstanding physicians and researchers. We have doubled the number of patients enrolled in clinical trials, and over a third of those patients are participating in Winship physician-led studies. Our hard work paid off this year when Winship was selected as one of 30 U.S. cancer centers to be a lead academic site in the National Cancer Institute’s new National Clinical Trials Network.
national leader in creating new diagnostic and therapeutic approaches to cancer.
Q:3
What is the most pressing issue in the cancer world? One of the most challenging issues we’re facing is in optimizing a personalized approach to cancer diagnosis and treatment. We are just learning how to ask the questions in this realm, let alone how to answer them. Genomics information related to a cancer diagnosis can be overwhelming. We are working with some of the best minds in the world to see how our discoveries in cancer genomics apply to the patients we see every day at Winship.
Q:4
What are some of the most promising developments happening in Winship laboratories? Some of our most exciting work is in the area of new drug and target discoveries. We’re one of only two NCI-designated cancer centers looking at protein-protein interactions in patients with brain tumors and one of several studying how to best target lung cancer mutations. Thanks to our partnership with Georgia Tech, we’re also a
Q:2
You wear a lot of hats at Winship, how do you find time for everything? This type of work energizes me. None of us view these responsibilities as a burden. They are opportunities. If any of us can make a difference, that just gives us more energy.
Q:5
What are your goals for the next five years at Winship? It’s simple. We want Winship to be the place where groundbreaking cancer discoveries translate into the very best care for patients with cancer.
2 Winship Magazine | winshipcancer.emory.edu 5 winship | in the news
3D MAMMOGRAPHY SERVICES OFFERED
Emory Healthcare is now offering the most advanced breast imaging technology available to be used in the early detection of breast cancer. Tomosynthesis, or 3D, mammography screening exams are available to patients at three locations: the breast imaging centers at the Winship Cancer Institute on Emory’s Clifton Road campus, Emory University Hospital Midtown and Emory Johns Creek Hospital
The 3D imaging technique has proven to be more accurate than conventional mammography at detecting breast cancers, and it produces fewer false-positives that result in patient call-backs for additional testing.

Emory Proton Therapy Center Update
Construction is more than half-way completed on the new Emory Proton Therapy CenterWinship Cancer Institute. The facility is due to open in midtown Atlanta in 2016, and will be the first of its kind in Georgia to offer patients access to the most advanced radiation technologies available.

Winship Cancer Institute of Emory University is one of the top 25 cancer programs in the nation according to 2014 rankings by U.S. News & World Report. The annual list ranks cancer care at Emory University Hospital through Winship the 24th best in the country, a 20-position jump from 2013.
Winship is the only cancer program in Georgia to be named in the top 50 in the country in the magazine’s annual survey of the nation’s best hospitals.
Winship Magazine | fall 2014 3
Torres Wins Komen Grant
Winship radiation oncologist







Mylin Torres received a threeyear, $450,000 research grant from the Susan G. Komen Board of Directors. The grant will support Torres’ work on research investigating the role of inflammation and fatigue during and after breast cancer treatment.
Torres, a Georgia native, completed her residency at the University of Texas, MD Anderson Cancer Center. She joined the Winship faculty five years ago as an attending physician and researcher. She focuses her efforts on providing outstanding patient care to women with breast cancer and is investigating therapy-related side effects like fatigue and depression.

Winship Website Unveiled
Winship Cancer Institute’s website has a new look, designed with patients in mind. You can easily access the website on the go from your smartphone or tablet.



Go to winshipcancer.emory.edu.


Rein Saral Retires
The Baltimore Sun headline from Feb. 15, 1991 said it all: “Hopkins’ loss is Emory’s gain.” After being recruited to head up the bone marrow transplant program here, Rein Saral began a long and fruitful career at Emory in July of that year. His mission: to greatly increase the number of transplants the unit was performing and to expand Winship’s translational research in transplantation to improve the procedure and its outcomes.
Saral retires this fall, having fulfilled his mission and then some. Today, Winship’s Bone Marrow and Stem Cell Transplant program performs nearly 400 transplants a year for patients with blood cancers and other diseases, making it the largest in the Southeast and one of the most experienced in the

country. Under Saral’s leadership, the Winship program has implemented advanced clinical practices that have resulted in better survival rates and reduction of side effects from transplantation.
Before coming to Emory, Saral was known for having pioneered the use of bone marrow transplantation for treating AIDS-related malignancies and sickle cell anemia and other inherited blood disorders. He also was the first to demonstrate effectiveness of a safe antiviral (acyclovir) therapy against herpesviruses in transplant patients. His influence at Emory has gone beyond the BMT program; he served as director of The Emory Clinic during a significant period of growth, and he helped Winship develop the infrastructure needed to achieve its National Cancer Institute designation, first awarded in 2009 and renewed in 2012. He is retiring as professor emeritus and will continue to serve Winship as a valued colleague and mentor.

4 Winship Magazine | winshipcancer.emory.edu winship | in the news
New Winship Leadership Positions
Jonathan L. Kaufman is the new medical director of Winship Cancer Institute’s Ambulatory Infusion Centers. Kaufman is responsible for coordinating care for over 10,000 cancer patients who receive infusion services at Emory University Hospital Midtown, Emory Johns Creek, Emory Saint Joseph’s Hospital and at Winship on the Clifton Road campus.

Kaufman is part of a collaborative team, which includes Sheryl Bluestein, director of Infusion Services. The team is focusing on streamlining and improving the patient experience while building on outstanding patient outcomes.
Suresh S. Ramalingam, professor of hematology and medical oncology, is the new co-leader of the Discovery and Developmental Therapeutics (DDT) program at Winship Cancer Institute. The DDT program aims to facilitate molecular target-based cancer drug discovery, biomedical technology and clinical trials for therapeutic development.

Ramalingam takes the place of Fadlo R. Khuri, deputy director of Winship and professor and chair of the Department of Hematology and Medical Oncology. Khuri, a founding leader of DDT, served in this role for 12 years.
Ramalingam joins Haian Fu, director of the Emory Chemical Biology Discovery Center, in co-leading the DDT program.
Melissa Gilbert-Ross is the new director for the Cancer Animal Models Shared Resource at Winship. The Cancer Animal Models facility assists investigators in developing and analyzing appropriate animal models for cancer research, providing a critical link between pre-clinical research and testing in humans.
Gilbert-Ross plans to build on the facility’s strength in genetically engineered mouse models to advance the development of personalized pre-clinical trials. She is currently developing an independent research project that uses a combination of drosophila (flies) and mouse genetics to elucidate how LKB1 mutations drive metastasis of non-small cell lung cancer in vivo.
LONG JOURNEY, STRONG BONDS
In her many years of battling colon cancer, Kate Winne has had five surgeries performed by Charles Staley, chief of surgical oncology at Winship, including the Hyperthermic Intraperitoneal Chemoperfusion (HIPEC) procedure that circulates heated chemotherapy directly into the abdominal cavity in order to penetrate cancerous tissue. Staley, Kate and her husband Mark Winne, veteran investigative reporter at WSB-TV and master of ceremonies for the Winship Win the Fight 5K, were featured in a recent story on WSB’s People 2 People program. The story explored the experience of long-term cancer treatment and the special bond that forms between patients, their families and their healthcare team.


Winship Magazine | fall 2014 5
PETE WINKEL

6 Winship Magazine | winshipcancer.emory.edu feature | team katie
Katie Groover was diagnosed with an aggressive form of multiple myeloma three years ago. She made up her mind about enrolling in a clinical trial at Winship Cancer Institute before she ever walked out of her doctor’s office.
STEPPING UP FOR Science
By Martha Nolan McKenzieR
obin Roberts was able to return to her host spot on Good Morning America. Melissa Etheridge was able to record more songs. Brandon Davis was able to go back to playing professional ice hockey. All these feats were made possible because somewhere, at some time, a patient enrolled in a clinical trial and received an experimental treatment for the first time.
“The many successful treatments we have for
was
to try a new drug in a trial,” says
Winship Magazine | fall 2014 7
cancer today are here because someone
willing
R. Donald Harvey, director of the Winship Phase I Clinical Trials Section. “Without clinical trials, we would not be able to move medicine forward.”
A clinical trial is a research study that tests new ways to prevent, diagnose or treat disease. Trials investigate promising new drugs, drug combinations, new approaches to surgery or radiation therapy as well as novel treatments such as immune or gene therapies. New treatments make it into clinical trials only after they have spent years undergoing development in the lab and testing in animals. Testing in humans is conducted in three phases (see sidebar on page 13) over many years before a new treatment can be approved by the U.S. Food and Drug Administration (FDA).
Pulling together everything involved in running a clinical trial takes a team approach. “An entire group needs to work together to run a trial, including basic scientists, clinician scientists, research coordinators, research nurses, pharmacists, and regulatory specialists,” says Bassel F. El-Rayes, associate director for clinical research and director of the gastrointestinal oncology program at Winship. “That’s what a cancer center like Winship does. It brings all these
people together under one umbrella.”
It’s something Winship does quite well. Since 2007, a whopping 75 percent of all new FDA approved cancer drugs have been tested through a Winship clinical trial. Fueled by the strong scientific research base at Winship and Emory University School of Medicine, 40 percent of all the trials here are investigator initiated. That means the drug or treatment being studied grew from the basic research of a Winship investigator. “Our investigators prefer to write their own studies and to be on the forefront of research,” says Harvey. “Having investigator-initiated studies is a focus of our research mission.”
Winship’s clinical trials program is growing steadily. In 2013, 760 patients were enrolled in 250 Winship clinical trials. This year, investigators hope to enroll over 800 patients. And Winship has been selected as a Lead Academic Participating Site for the National Cancer Institute’s (NCI) new National Clinical Trials Network (NCTN). The NCTN will serve as NCI’s primary infrastruc-

8 Winship Magazine | winshipcancer.emory.edu feature | team katie
“Do not sign this consent form unless you have had a chance to ask questions and get answers that make sense to you.”–
Winship/Emory clinical trials consent formClinical trials participants often form strong bonds with their care team members. R. Donald Harvey and Carolyn Higgins have known each other for years.
ture to conduct Phase II and III cancer clinical trials. NCTN clinical trials will enroll over 17,000 patients per year with a variety of cancer types and from diverse backgrounds
The clinical trial work done at Winship is critical to advance the treatment of cancer. “There are very, very few diseases out there for which we feel we have the best treatment possible,” says El-Rayes. “There is always room for improvement, especially in cancer treatments. Clinical trials are the way for us to either improve outcomes or produce the same outcomes with fewer side effects.”

Despite the importance of clinical trials, only about 5 percent of adults with cancer enroll. Why? Reasons vary, including lack of knowledge of trials, access to care, feeling it’s a last resort, fear of getting a placebo and perception of being a human guinea pig. While participating in a clinical trial may not be the right choice for every patient, it’s critical to make the decision based on facts rather than myths.
The first obstacle – lack of awareness – is easily overcome. It’s true that patients usually are referred to trials by their doctors, but you can ask about trials if your doctor doesn’t bring it up. You can also search for trials yourself at ClinicalTrials.gov, a service of the U.S. National Institutes of Health. There are clinical
trials for almost every type of cancer and stage of disease so a little digging might turn up an appropriate trial.
The feeling that clinical trials are only an option after all other treatments have failed is misplaced. While some people do enroll after other treatment options have been exhausted, others consider trials right from the outset. That’s the decision Cindy Sullivan made. When the Athens woman was diagnosed with multiple myeloma in 2008, a year after her daughter’s birth, she was given two options. She could get standard treatment in Athens, or she could commute to Atlanta to participate in a Winship clinical trial testing a new combination of drugs. “When I heard about the clinical trial, I knew that’s what I wanted to do,” says Sullivan, now 46. “I didn’t want to look back and regret that I hadn’t done everything I could.”
Fears of getting a placebo are also misguided. In cancer clinical trials, you will either get standard of care – what is generally considered to be the most effective treatment available – or the new treatment being studied. “The only time a placebo is used in a cancer trial is when there is no standard of care,” says El-Rayes.
And far from being treated as a guinea pig, clinical trial participants are seen as heroes by the medical team and are given the utmost respect. Indeed, you will likely get more attention from
Winship Magazine | fall 2014 9
Kathleen Rodger and Bassel El-Rayes oversee the 250 clinical trials underway at Winship.
your health care team and more careful monitoring of your condition and the possible side effects of treatment if you take part in a clinical trial. And participation can be empowering, giving you the feeling you are playing an active role in your care and helping others who will come after you.
The opportunity to pay it forward is what motivated Katie Groover to enroll in a clinical trial. Groover was diagnosed with an aggressive form of multiple myeloma in 2011. Her doctor referred her to Sagar Lonial at Winship because she was aware he was involved in many clinical trials. “Dr. Lonial spent an hour and a half with my husband and me explaining about the trial and told us to go home and think it over, but I had pretty much made up my mind before I walked out of the office,” says Groover, now 54. “The Lord has been good to me and I see
being in a clinical trial as a way to give back. I’d like to think I was able to help advance medicine to find a cure for this cancer.”
There are many other things to consider when weighing whether or not to enroll in a trial. You may be getting a treatment that has not been tried in humans before or been used for your type of cancer. That’s a risk that can cut both ways – if the new treatment turns out to be effective, you’d be among the first to receive it and benefit from it. On the other hand, if it turns out to have unanticipated side effects, you could suffer those.
Paul Hansen has experienced both sides of the equation. When Hansen’s non-Hodgkin lymphoma came back in 2010 after two earlier rounds of chemotherapy, he enrolled in a Winship Phase I trial. The treatment was ineffective against his cancer, so he started

10 Winship Magazine | winshipcancer.emory.edu feature | team katie
“When I heard about the clinical trial, I knew that’s what I wanted to do. I didn’t want to look back and regret that I hadn’t done everything I could.”
– Cindy Sullivan, multiple myeloma patientAnne Kilpatrick counted on her doctor, Christopher R. Flowers, for support while she was in a clinical trial for lymphoma treatment.

Winship Magazine | fall 2014 11
ANN BORDEN
Cindy Sullivan with nurse practitioner Charise Gleason. Sullivan is in a trial testing a new combination of drugs.
feature | team katie
 Phil Williams (right) calls Winship radiation oncologist Jonathan Beitler a hero for helping him survive stage IV head and neck cancer.
Phil Williams (right) calls Winship radiation oncologist Jonathan Beitler a hero for helping him survive stage IV head and neck cancer.
another chemo regimen that put him in remission. When the cancer returned in 2013, it took the form of very rapidly growing tumors all over his body. He enrolled in another trial, and this one worked like a miracle. “It was just unbelievable,” says Hansen, now 62. “You could practically watch the tumors shrinking. I’m in total remission right now.”
Phase I trials are testing drugs for which, to date, information on side effects in humans is limited. During the trial, patients are very closely and frequently monitored to ensure safety. Some are checked every 15 minutes while the drug is being administered. While historically, first-in-human Phase I trials have been reported to benefit only about 10 percent of participants, either by eliciting remission or shrinking a tumor, Harvey contends the benefit is understated. “If you go into a trial and your tumor stays the same size rather than shrinks, that’s considered not responding to the treatment,” says Harvey. “But I would consider it a win for the patient, particularly if they had very few side effects. It means we’ve stopped the growth of the cancer. If you are feeling well, that’s the beginning of the definition of a chronic disease. If you can take a drug or a combination of drugs that cause very few side effects and keep the cancer at bay, that’s a chronic disease, just like high blood pressure or high cholesterol. And we’re getting there.”
Participating in a trial generally gives you access to top cancer doctors and scientists, and your treatment is closely monitored by an entire team. On the other hand, you will likely need to make more frequent and longer visits and submit to more testing. “We ask a lot of our patients, particularly in our Phase I trials,” says Harvey. “We ask many times that they come to our center six or seven times in a three to four-week period. We ask that they spend upwards of 10 hours with us so we can give drugs, collect blood samples and assess how they are feeling. We ask that they perhaps drive long distances to Atlanta and maybe stay overnight. Our trial participants are phenomenally courageous and giving of their time.”
Cost likely will not be an issue when considering a trial, as long as you have insurance coverage. As a general rule, your insurance will pay for anything that you would have gotten as standard of care, and the trial generally covers all expenses related to the research. “A patient needs to check with his insurance company and find out what will be covered,” says Kathleen Rodger, director of the Clinical Trials Office at Winship.
Of course, if you do want to participate in a trial, you must first qualify. Every trial has certain specific conditions that must be met. Eligibility criteria can include treatment history, other medical conditions and type and stage of the disease.
In addition, you need to be in good condition, meaning you are still up and about and able to do most things for yourself. “We want to make sure the trial is safe for the patient,” says Rodger. “Trials generally look for people who are healthy enough to tolerate treatment.”
What the Phases Mean
Phase I trials study whether a new treatment is safe to use over a range of doses. Sometimes a drug is being used for the first time in humans. The treatment may be given to people with different types of cancers. A Phase I trial is mainly a drug safety study and tends to be small, enrolling around 20 patients.
Phase II trials study how well a treatment works for a certain cancer. These trials may include between 25 and 100 people. After a drug (or procedure) is found to be effective in treating cancer in a Phase II trial, a Phase III trial will study it further.
Phase III trials compare the new drug or procedure to accepted standard treatment to see which works the best. Phase III trials may look at different doses of the same drug, different drug combinations or different sequences of giving drugs. In these trials, people are randomized to get either the new treatment or the standard treatment. Phase III trials are large, enrolling hundreds or sometimes even thousands of participants.
And some trials are adding another type of criteria – looking for biomarkers that are believed to predict the likelihood that the drug being tested will be effective on you. “We’ve now added a layer of screening into the trial,” says Harvey. “Not only do patients have to be physically fit, they have to be molecularly fit. This is done with the hope that we’ll have more targeted therapies and more personalized approaches.”
A personalized approach is exactly what Winship is striving for. Indeed, one of Winship’s distinguishing characteristics is a dedicated Phase I unit. “We not only have a dedicated space, we have dedicated personnel and a dedicated culture,” says Harvey. “For example, we draw all the labs here. The physicians come to see the patients here. EKGs are done here. Our goal is to make this a truly patient-centered experience.”
It certainly was for Groover. “We called it the VIP room,” she says. “I had the same nurses and technicians every time I went, and everything was brought to me.”
But perhaps the thing that stands out the most for Winship trial participants is the level of caring they received. “I honestly can’t say enough good things about the people who treated me at Winship,” says Sullivan. “I actually became great friends with some of those nurses. They understand you are not a number – you are a person with a life and hopes and dreams. They truly care about you when you are there, and it makes a difference.” W
Winship Magazine | fall 2014 13
The first goal of cancer treatment is to fight the cancer. But patients quickly find their true motivation in this fight is to live and thrive, whether that means returning to the passions they pursued before diagnosis, or taking up new endeavors and setting off on new adventures.
Here are just four of the many Winship patients, and their doctors, who embody the spirit of hope.
ZFaces of Hope
14 Winship Magazine | winshipcancer.emory.edu feature | pursuing life featu
Photo essay by Jack Kearse
Anna Berrier knew that life as a paleskinned redhead put her at risk, so when a suspicious mole popped up behind her right knee, she went straight to melanoma surgeon Keith Delman. The energetic 20-something, who now has a clean bill of health, is not afraid to strap on her heels and show off her 6-inch scar.

Winship Magazine | fall 2014 15
Z
Firefighter Frank Summers has dedicated his career to saving lives, but he turned to Jonathan Beitler for lifesaving treatment for head and neck cancer. After completing radiation therapy, Summers was happy to ditch his treatment mask and get back into the gear that connects him to his passion.

16 Winship Magazine | winshipcancer.emory.edu
Muriel Smith is ready to get her game on after more than a decade of treatments for breast cancer. When the high school teacher and cheerleading coach proposed taking up tennis to help get back in shape, she leaned on her doctor, Amelia Zelnak, who urged her to go for it!

Winship Magazine | fall 2014 17
Two years after his bone marrow transplant, leukemia survivor Bob Falkenberg set off on a 1,700 mile bicycle trip to celebrate his good health and raise money for cancer research. Amy Langston was at his side for 100 miles of the trip. It’s been five years since the transplant, and Falkenberg is still in the saddle.

18 Winship Magazine | winshipcancer.emory.edu
Z
Every cancer is personal
Winship clinicians and scientists are developing new treatment options for lung cancer with regimens personalized to each patient.
By Sylvia WrobelSuresh S. Ramalingam and Fadlo R. Khuri are determined to translate gene mutation research discoveries into new, more targeted therapies for the patients they see every day.
Larry Dry’s lung cancer was discovered by accident. The husky, physically active 69-year-old had no cough, no breathing problems, only a little tingling in one hand. When his doctor ordered an X-ray before surgery for a pinched nerve, he wasn’t thinking lung cancer. Dry hadn’t smoked in 40 years and a chest X-ray taken less than a year earlier had been perfectly clear. But the new X-ray contained ghostly images of large nodules. Non-small cell lung cancer. Stage IV, the most advanced kind. Eight months of gut-wrenching chemotherapy shrank the tumors, but they quickly rebounded. A second, less toxic drug didn’t work.

Z
feature | lung cancer
Kathy Dry, a former CDC employee, asked the doctor if there wasn’t something else for her husband, perhaps something at Emory. And that was how, in July 2013, Dry met Winship Cancer Institute oncologist Suresh Ramalingam, professor and director of Winship’s Lung Cancer Program. Dry quickly entered one of the 20 to 30 ongoing lung cancer clinical trials underway at Winship, thanks to Winship’s status as Georgia’s only National Cancer Institute-designated cancer center. Dr. Ram, as his
Some genes suppress lung tumor activity. These slides show lung cancer cells (each blue area is a nucleus inside one cell) and a tumor suppressor gene, dyed green. The red areas are a protein produced by the cancer cells that helps them move.

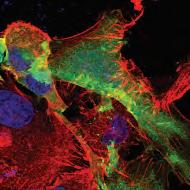
Courtesy of Winship’s Integrated Cellular Imaging Core.
patients call him, is principal investigator of a multi-institutional Phase II trial testing the efficacy of a new class of immunotherapy cancer drugs, drugs that stimulate the immune system to attack cancer cells while sparing healthy ones.
Every two weeks, Dry met with Ramalingam and Colleen Lewis, nurse practitioner in Winship’s busy clinical trials unit, and spent an hour in Winship’s infusion center. A huge benefit of the new immunotherapy treatments, says Ramalingam, is how well they are tolerated. Dry’s previous chemotherapy caused constant diarrhea. The new treatment only caused occasional gastrointestinal upset and he was able to regain lost pounds and his trademark energy. His tumors shrank by more than half and stayed that way for 11 months.
Thanks to their experience at Winship, Kathy Dry encourages people with lung cancer not to give up. There is hope, she says.
And more hope keeps coming, as Winship clinicians and scientists work with their research partners across campus and the country to design, develop, and test new, personalized treatment regimens. Increasingly those regimens are specific to each patient, such as strengthening an individual’s own immune response, as with Dry, or identifying and honing in on the different genes involved in an individual’s cancer or response to treatment.
Making it personal
Lung cancer is by far the leading cause of cancer death in men and women. But lung cancers – even specific types such as small-cell or non-small cell lung cancers – are not all the same. That’s why, when lung cancer patients arrive at Winship, a small tissue sample of their tumor undergoes genomic screening to determine which gene has gone awry, driving that individual’s cancer.
For example, among recently screened Winship patients with lung adenocarcinoma, a sub-type of non-small cell lung cancer, approximately 50-60 percent could be placed into a specific molecular genetic subcategory. “Knowing which gene is malfunctioning gives us a highly personalized target for treatment,” says Ramalingam. “Our overarching theme in combating lung cancer at Winship is divide and conquer.”
Targeting genes
The genetic testing panel studied for lung adenocarcinoma includes approximately 48 genes. Winship scientists are expanding that list with treatments to match. Take, for instance, the gene LKB1, mutated in 30 percent of all non-small cell lung cancers. This subgroup has a higher risk for metastasis, the process responsible for most cancer deaths. Adam Marcus, director of Winship’s Integrated Cellular Imaging Core, uncovered how the LKB1 mutation promotes tumor spread. One possible answer is that once LKB1 mutates, it activates a flurry of production of
feature | lung cancer featu 20 Winship Magazine | winshipcancer.emory.edu
a type of protein called focal adhesion kinase or FAK. Another gene, named KRAS, may initiate the original tumor, but when KRAS joins forces with mutant LKB1 and the hyperactive FAK proteins go to work, the tumor can spread.
In addition to shedding valuable light on how metastasis works in any type cancer, Marcus and Winship’s multidisciplinary team – oncologists, pathologists, cell biologists, pharmacologists, molecular geneticists, biostatisticians, and others – are working to help this particular subgroup of patients. It’s divide and conquer in action, here and now.
The first step was to add LKB1 to Winship’s genomic screening panel. Second was to develop and test the first-ever treatment to inhibit the growth-promoting FAK proteins produced by the mutated LKB1 gene. In collaboration with pharmaceutical companies and other research institutions, Winship is planning a phase II clinical trial, involving Ramalingam, Winship Deputy Director Fadlo R. Khuri, and geneticist Wei Zhou. The new trial will show how well the treatment works in patients with mutant LKB1. Marcus believes targeting hyperactive FAK in LKB1-mutant patients will prevent new metastases, leading to more “progression-free survival.”
Haian Fu is a pharmacologist at Winship and head of Emory’s Chemical Biology Discovery Center. He has some powerful allies and tools in his laboratory that are leading to the development of new lung cancer therapies.

Targeting vulnerability along the genetic pathway
Not all genes are as so obligingly evident. Others are considered “untargetable.” For example, when a mutation causes what scientists call gain of function, therapies can be designed to inhibit this activity. Loss of function mutations – such as those that inactivate tumor suppressors – present additional challenges. But those are challenges the Winship team is finding new ways to meet.
Pharmacologist Haian Fu takes a network approach. Genes work through the proteins they create. And since protein-to-protein networks
Winship Magazine | fall 2014 21
act as signal relay systems, the effect of a single mutated gene can alter the activity of genes along the network pathway, transmitting signals that drive tumor development and progression.
Several years ago, Fu began to focus on 14-3-3-zeta, a gene that controls cell division, growth and death in most living things. It can go into overdrive in lung cancer, however, markedly lowering survival. Understanding the gene’s complex regulatory/signaling role has allowed the researchers to identify a series of cancer-associated proteins controlled by 14-3-3-zeta. Discoveries in the past few months alone include both tumor suppressors and tumor promoters, all players in lung cancer, all vulnerabilities that can be targeted and disrupted.
Creating the right bullet for each target
When it comes to developing novel therapeutic strategies for lung cancer, Fu and his lab have two important allies. One is long-time research collaborator Fadlo R. Khuri, chair of the Department of Hematology and Medical Oncology and Roberto C. Goizueta Distinguished Chair in Translational Cancer Research and a leading physician and clinical investigator in lung, head and neck and aerodigestive cancers. Fu says Khuri’s commitment to his patients never lets the team forget the importance of what they are doing. Fu’s second ally is the robotassisted high-throughput screening technology in the Emory Chemical Biology Discovery Center, which Fu heads. Highthroughput screening assays – immensely powerful tools that collect in minutes massive amounts of data that required months to collect only years ago – allow him to screen many thousands of compounds, looking for the half of one percent of compounds with the potential to reverse the cancer-promoting genetic changes along the pathway. A number of these compounds are now in development as potential new lung cancer therapies.
Creating a therapy sum greater than its parts
Other studies at Winship, often in partnership with the National Cancer Institute (NCI), its collaborative networks, and pharmaceutical companies, show what happens when traditional chemotherapy is enhanced with inhibitors of specific genes. An example: one goal of chemotherapy is to slow down rapidly multiplying cancer cells by damaging their DNA. Adding an agent that inhibits production of DNA repair proteins further weakens the cancer cells, making chemotherapy more effective.

If genomics is the current big thing in lung cancer advances, the next big thing, says Ramalingam, is likely to be using immunotherapy to treat cancer and studies to determine which traditional, genomic, immunotherapy or combined approaches work best for which genetic subgroup of patients. In fact, genomics is restoring the good name of some drugs that had not appeared
very effective when results were tallied for all lung cancer patients as a group, but now prove extremely effective for specific genetic subgroups.
Ramalingam says “Winship is determined that each of our patients with lung cancer gets the best treatment to combat his or her unique disease. And we are equally determined to find new ways to do just that.” W
feature | a team approach featu 22 Winship Magazine | winshipcancer.emory.edu
feature | lung cancer
Adam Marcus is director of Winship’s Integrated Cellular Imaging Core. He discovered how a gene that mutates in 30 percent of all non-small cell lung cancers promotes tumor spread.
Smoke-Free Homes
Living with smokers increases nonsmokers’ chances of developing lung cancer by 20 to 30 percent.* But smoking inside is permitted by half of all homes with a smoker, even more in lower income households. A National Cancer Institute-funded study headed by Rollins School of Public Health’s Michelle Kegler suggests most of those households are receptive to going smoke free and, with some simple help, can succeed.
In the summer of 2013, more than 4,000 callers to the United Way of Greater Atlanta’s 211 call center were directed to the help they requested and were then asked a smoking-related question: did anyone regularly light up in the house? If yes, would they like to participate in a program to help them make their home smoke free? Eighty percent jumped at the chance. Three months later, 30.4 percent of those given materials and a coaching phone call from Emory Prevention Research Center staffers had earned their “smoke-free home” window sticker.
Like New Years’ resolutions, behavioral changes often fade away. This one strengthened. After six months, the number of smoke-free homes had climbed to 40 percent.
As is standard in research determining intervention efficacy, half of participants received no materials or coaching, only 30-minute phone calls collecting data on secondhand smoke exposure in their houses. These phone calls alone were enough to nudge 14.9 percent of households to go smoke free at three months, rising to 25.4 percent by six months.


Emory’s research partners at the University of North Carolina and University of Texas-Houston are now testing the intervention, using 211 agents instead of university staffers. If it works as well in their communities as in Atlanta, Washington University in St. Louis will expand the grant nationally in collaboration with Emory and other partners. W
*According to the US Surgeon General, www.cancer.gov/cancertopics/factsheet/ Tobacco/ETS#r4, which in turn references U.S. Department of Health and Human Services, “The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General.” Rockville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2006.
Winship Magazine | fall 2014 23
Michelle Kegler, Winship member and Rollins School of Public Health researcher, found a way to make more homes smoke free.
Smoking inside is permitted by half of all homes with a smoker, even more in lower income households.
FREEZER Finding answers in the

24 Winship Magazine | winshipcancer.emory.edu
By Sylvia Wrobel
Winship set out to build a more comprehensive breast tissue bank in 2010. Today, Emory’s breast tissue procurement and banking program, designed by three of Winship’s leading breast cancer researchers and funded by the Wilbur and Hilda Glenn Family Foundation, has greatly expanded and is enabling researchers to more easily and more quickly find the breast tissue they need to move forward.
Expanding breast tissue collection and storage
Collecting and banking tissue of patients is not new. For years, surgical oncologists have taken tissue specimens during biopsies or operations to remove a tumor, tissue samples that allow them to make a diagnosis and, if found to be cancerous, to determine tumor type, size, and characteristics. They also use tissue specimens to make sure the margins (edges) of the excision are clean, meaning no cancer cells have been left behind. Part of the tissue sample is then stored, available if
later needed by the clinician, perhaps to compare to a second tumor.
Diagnosis and treatment of the individual patient always will be the primary use for tissue samples, but researchers know the tissues also hold answers for all breast cancer patients. In the past, only a small percentage of tissues was available for research. Now, nearly all breast cancer patients seen at Emory are being asked if they will consent to having tissue left over from their clinical procedures be made available for use by breast cancer researchers.


“Almost all of them agree,” says Sheryl Gabram-Mendola, expert in the surgical treatment of breast cancer for Winship and Grady Memorial Hospital. “There is no downside, and most women are eager to help other women who have or may develop breast cancer.”
Working with Gabram-Mendola to grow the program are Paula Vertino, head of Winship’s Cancer Genetics and Epigenetics program, and Ruth O’Regan, director of translational breast cancer
Winship Magazine | fall 2014 25
If you’ve had a biopsy or surgery connected to a breast cancer diagnosis at Winship, chances are you were asked to allow some of your left-over tissue to be used in Emory’s breast tissue bank. If you consented, you are helping researchers here and all across the country find answers to improving diagnosis, treatment, even prevention of breast cancer.Surgeon Sheryl Gabram-Mendola helped design and implement a system to collect breast tissue samples and data from three clinical sites. Winship’s Director of Translational Breast Cancer Research Ruth O’Regan oversees the design of clinical trials using breast tissue data.
feature | breast cancer
research and a physician with a major interest in triple negative breast cancer. It’s a good team. Gabram-Mendola helped build a system for consistently collecting tissue samples and data across three clinical sites. Vertino and her team of genetic researchers make sure other scientists know the tissue is available and they facilitate its appropriate use. O’Regan oversees the design of clinical studies using the data. The recent establishment of the Glenn Family Breast Center at Winship helped further boost the breast tissue bank program and a range of related research projects.
The tissue bank collection/consent mechanism is now in place at Emory University Hospital, Emory University Hospital Midtown, and the Avon Breast Center at Grady Memorial Hospital. Research coordinators approach over 90 percent of Winship breast patients to get permission to use their tissue samples in studies, now or in the future.
It works this way. When a patient is having a procedure, a research project coordinator at the site explains to her how researchers use the left-over tissue and asks if she would be willing to sign a consent form allowing her tissue to be available to them. If she says yes, the clinician places the extra cells in a glass tube and hands them to the coordinator, who is waiting outside the procedure or operating room. The coordinator then processes and freezes the cells. Thanks to a sophisticated data management system created for the tissue bank, patients are identified only by numbers to protect their confidentiality, but each tissue sample is linked to a large database of information about the patient, such as age, weight, medical history, and behaviors like smoking, alcohol use, and exercise.
This is a model also used at other National Cancer Institute-designated cancer centers, part of a movement toward precision medicine: being able to combine hun-
dreds, even thousands of bits of cellular, clinical, genetic, environmental, behavioral and other information to allow research-
ers and clinicians to better understand an individual’s cancer and identify the exact “personalized” medical treatment that will work best for that individual.
Winship is at the cutting edge of this trend, says Gabram-Mendola. In addition to collecting cells from an initial breast cancer, as is common, it also collects and stores normal cells (40 percent of breast biopsies turn out to be negative for breast cancer) and – even more visionary – metastatic cells: breast cancer cells that have spread to other organs, such as the lungs, bones, or liver.

What also makes Winship’s tissue bank especially valuable is its size and make-up. More than 1,000 breast cancer patients are seen per year at the three sites, and, given Atlanta’s demographics, especially at Grady, a higher than average proportion of patients are minorities – African Americans, Latinas, Asians, and others who too often have not been well represented in research studies.
“We already had some of the pieces of a good tissue bank program,” says GabramMendola, “but we needed a system-wide patient database and a robust information technology system to connect pathology and clinical data. The gift from the Glenn family, long-time supporters of Winship, allowed us to build that. Having the breast cancer tissue bank and database makes our researchers more competitive for NCI and other research funding and better able to tackle the complexities of breast cancer.” W
26 Winship Magazine | winshipcancer.emory.edu
“There is no downside, and most women are eager to help other women who have or may develop breast cancer.”
– Sheryl Gabram-Mendola, breast cancer surgeonPaula Vertino heads up a team of genetic researchers working with data gathered from breast tissue samples that will allow them to better understand and treat an individual’s cancer.
Focus on Philanthropy
Gifts to Winship support cancer research happening right here in Georgia. That research is being translated from lab bench to bedside, benefiting tens of thousands of patients every year. Here’s how we did in fiscal year 2014.
Total donors
7,733
Total gifts
9,858
Donors can contribute to nearly two dozen cancer research funds at Winship. For more information, go to: winshipcancer.emory.edu/support
Total dollars raised
$11,218,047
Winship Magazine | fall 2014 27
SARCOMA Bone Marrow Transplant Brain Tumor Breast Colon Rectal Ovarian ENDOMETRIAL CERVICAL Head & Neck Leukemia Lung Lymphoma Melanoma Multiple Myeloma EYE Pancreatic Liver Prostate Clinical Trials Bladder Kidney
We have some great Friends!
Friends of Winship had a busy year helping to build community understanding and awareness of the advancements in cancer research at Winship. Started four years ago, Friends of Winship hosts two educational events every year that feature Winship physicians and researchers highlighting different cancers. The group also had tremendous success in raising funds that will benefit cancer research at Winship.
Friends of Winship hosted the “Fashion a Cure” fundraising event that brought together 16 local boutiques to coordinate fashions modeled by cancer survivors and others affected by the disease.



The third Winship Gala, held at the Piedmont Driving Club, celebrated the courage displayed by patients, families, physicians and researchers in facing and treating this disease.



winship | support
Leaders of Friends of Winship: standing left to right, Founding Co-Chairs Marietta Petters and Kathy Bowman; seated left to right, Incoming Co-Chairs Missy Craver and Julie Fox.
Members of the Fashion Show Committee, from left to right: Susan Simpson, Julie Fox, Fashion Show Chair Ada Lee Correll, and Laura Palickar
One of the models at the “Fashion a Cure” show.
Walter J. Curran, Jr., Julie Levine, Amy Kreisler, Fadlo R. Khuri.
28 Winship Magazine | winshipcancer.emory.edu
Honorary Chairs, Lynne and Howard Halpern.
Big Win at the Winship Win the Fight 5K

The fourth annual Winship Win the Fight 5K on September 27th drew more runners and sponsors and raised more money than any previous year. In fact, thanks to the many teams and individual supporters who came out for the race or donated from afar, the Winship 5K surpassed its goal of raising half a million dollars. Cancer survivors, families, Winship physicians, nurses and support staff, and supporters of all kinds made up the spirited crowd of participants who walked, ran or cheered from the sidelines at this inspiring community event.



Winship Magazine | fall 2014 29

1365-C Clifton Road N.E. Atlanta, GA 30322 winshipcancer.emory.edu 1-888-Winship