










|
 |
| |
|
|
 |
 E-mail
to a Friend Printer
friendly
E-mail
to a Friend Printer
friendly |
|
| |
|
|
| |
By
Sherry Baker |
|
| |
|
|
| |
Carroll
Payne feels better than he has in years.
That wasn't the case last July, when he suffered a major
heart attack after working in his yard in the hot Georgia sun.
Today, the 53-year-old Payne is back on the job as a fire battalion
chief in suburban Gwinnett County. He resumed his life and livelihood
of 33 years after being treated for myocardial infarction (MI)
at Emory Crawford Long Hospital. Payne's life is different
now. He has a stent in his coronary artery and takes medication
to prevent his blood from clotting. He no longer eats red meat
or fried foods. He exercises regularly. And he is involved in
a groundbreaking clinical trial to determine whether the adult
stem cells in his body—the cells that renew themselves to
become specific types of cells—can be manipulated to heal
his damaged heart. |
|
| |
|
|
| |
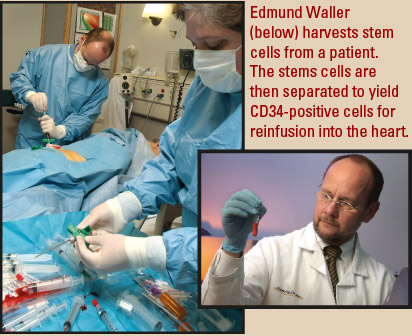
The
physicians leading the study are hopeful that the stem cells harvested
from the bone marrow in Payne's hip will promote formation
of new blood vessels to improve heart circulation and enhance function.
While many patients recover at least
partially from heart attacks, approximately 70% suffer permanent
damage because the artery blockage causing the attack keeps oxygen
from reaching parts of the heart muscle. Currently, no treatment
is available to restore function in damaged heart muscle, including
those patients on the brink of heart failure.
Emory cardiologist Arshed Quyyumi
and hematologist Edmund Waller believe that may change, based on
previous studies in Europe showing that infusing stem cells into
the heart after heart attack improved heart function. They are directing
the Emory arm of a multi-center Phase I/II clinical study in which
stem cells harvested from bone marrow are reinfused into patients
through cardiac catheterization. The Texas Heart Center, Vanderbilt,
and Atlanta's Piedmont Hospital are partnering with Emory
as well. |
|
| |
|
|
 |
| |
|
|
| |
A
‘renewed' way of thinking
The idea that the damaged heart can be "renewed" is
the result of an extraordinary paradigm shift that occurred in medicine
over the past decade. It didn't garner loud headlines like
heart pacemaker recalls or unexpectedly serious drug side effects.
Nor did it spur TV news and radio debates like the Terri Schiavo
case or the political controversy over embryonic stem cell research.
In fact, it has been overlooked by
a lot of people, including many in the medical community. But its
repercussions may forever change the concept of how the human body
can be healed.
"In the past, cardiology focused
on finding out where injuries were and using surgery to repair them
when possible, as well as identifying risk factors," says
Quyyumi. "But we now realize that hearts and blood vessels
can be regenerated.
"We now know that the endothelium
is continually dying and being replaced, and we also understand
how this turnover occurs—from progenitor cells, or adult stem
cells, most of which come from bone marrow."
How well an individual's body
is able to turn over cells and adequately repair blood vessels may
well depend on possible factors for cardiovascular disease, such
as high cholesterol, high blood pressure, smoking, and diabetes.
"These are paramount in terms of what causes atherosclerosis
and, ultimately, heart attacks," says Quyyumi. "Now
we believe the bone marrow's ability to replenish the endothelium
and stop atherosclerosis from occurring probably is affected by
the same risk factors that can damage blood vessels." |
|
| |
|
|
| |
 |
|
| |
|
|
| |
How
many stem cells does it take?
The process of manipulating the body's own progenitor cells
to spark or speed up repair of blood vessels and heart muscle has
worked in animal models, Quyyumi points out. In a handful of human
trials, some but not all of the studies showed positive benefits.
"All have shown that it is a
safe thing to do—there were no obvious dangers or downsides.
But the benefit, how much recovery and function is occurring, has
varied among trials," he says. "We suspect the variation
has a lot to do with timing and dosing. This is part of a series
of studies designed to refine the technology and define what will
work."
To that end, researchers are investigating the infusion of progenitor
cells into the coronary arteries of recent MI survivors in ways
never studied before. For example, in previous studies, researchers
have used all of the bone marrow cells or a fraction of smaller,
mononuclear cells without knowing specifically what type was being
given to MI survivors.
In the Emory study, researchers are
isolating a specific population of cells from bone marrow for infusion
into heart muscle. "These are CD34-positive cells—mononuclear
white blood cells that are enriched with a population of stem cells,"
says Waller, who directs the Bone Marrow and Stem Cell Transplant
Center. "These cells can restore normal bone marrow function
when we transplant them into patients with leukemia. We think the
same cells may be therapeutic in repairing blood vessels and damage
to the heart."
This trial, unlike previous ones,
is a dose-response study. Each group of 10 patients (40 in all)
receives a randomized titrated dosage of 5, 10, 20, or 30 million
CD34-positive cells.
"A lot of earlier studies used
very small bone marrow aspirates and relatively small doses of cells,"
says Quyyumi. "We are giving larger numbers to discover if
there is a threshold beyond which there may be a benefit not seen
in previous studies." |
|
| |
|
|
| |
 |
|
| |
|
|
| |
Timing
may be everything
As Waller notes, cancer specialists are well aware that stem cells
found in the bone marrow can be induced to enter the blood circulation
through drug therapy. So why not use the same drugs to help move
stem cells to help heart attack patients, instead of physically
removing the cells via aspiration and reinfusing them?
"These drugs cause the white
blood count to go up considerably and that can help cancer patients,
but their use for heart attack patients has been associated with
adverse events related to reocclusion of coronary vessels,"
Waller says. "It might be dangerous to mobilize the blood
cells so soon after heart attack."
In fact, timing may be crucial to
successfully using stem cells to help repair hearts. For the Emory
study, initial testing and aspiration and reinfusion of cells are
done within the first nine days after a heart attack.
"There might be a narrow window
of opportunity when we think these cells must be injected for them
to be effective," Quyyumi explains. "We don't
know yet how long that time period is or whether it can be extended.
But we do know we can't do this effectively a day or so right
after the MI. It appears not to be efficacious, probably because
of the extensive inflammatory reaction that occurs after the MI,
which makes the environment uninviting for stem cells to grow. However,
five or six days afterward seems to be the optimal time we are aiming
for. At this time, previous researchers have also observed benefits."
Recent MI patients are still being
recruited for the study. Thus far, the first cohort of patients
has been treated with 5 million CD34-positive cells. During the
90-minute bone marrow harvest procedure, the longest part of the
study process for patients, Waller collects a number of small aspirations
of the bone marrow. The goal is to achieve a product that is mainly
bone marrow cells with little blood.
The cells are shipped immediately
to Amorcyte, the biotech company that is funding the clinical trial,
in New Jersey. Amorcyte separates the CD34-positive cells and ships
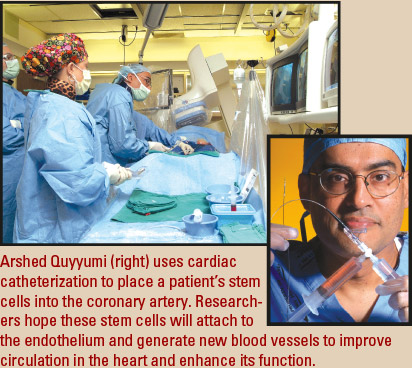
them back to Emory within 24 to 36 hours. During cardiac catheterization,
the stem cells are placed in the coronary artery where a blockage
caused the patient's heart attack.
"A portion of the stem cells
is infused, and then a balloon is inflated around the catheter,
sealing off the artery from any other blood flow," Quyyumi
explains. "After a minute, normal blood flow is allowed to
resume, and the process is repeated until the entire dose of cells
is injected into the affected artery. The hope is that the stem
cells will ‘home' or attach to the endothelium.
"There may be many factors that
explain the potential benefits of this technique. We believe the
cells initiate angiogenesis, which improves heart function by getting
more oxygen to the heart. There is also evidence that they may prevent
further dilation of the heart and prevent development of congestive
heart failure."
Follow-up with patients is important
to learn whether the stem cell transfer is as beneficial as expected.
At three months and again at six months, patients undergo an MRI,
nuclear scan, and echocardiogram to measure heart function and perfusion
to document how well blood is reaching the damaged area of the heart.
Patients will return for additional follow-up of these markers and
an exercise test at one year. Long-term follow-up is slated for
five years. |
|
| |
|
|
 |
| |
|
|
| |
Pushing
the envelope
Quyyumi believes that CD34-positive cells are much more likely than
nonspecific bone marrow cells to become endothelial cells that improve
circulation and function of the heart. But he has his eye on what
may become the ultimate goal for this type of research—the
creation of new heart muscle cells using a stem-cell type that replenishes
the cardiac cells that died as a result of a heart attack.
In a previous study, Quyyumi and Waller
successfully mobilized cells from the blood marrow to improve circulation
in patients with peripheral vascular disease. Eventually, adult
stem cells may prove helpful in treating other cardiovascular problems,
including heart failure caused by cardiomyopathy and angina in patients
beyond treatment with angioplasty and/or bypass surgery. Notes Waller,
"The bone marrow is a rich source of adult stem cells that
appear to be able to help repair a number of different tissues."
"Stroke is another area where
this kind of technology, once it is refined, has great promise,"
Quyyumi adds. "This is just the beginning, and much basic
science research still needs to be done, but a lot of clinical translation
is now occurring. The NIH has been a driving force in terms of funding
this research in the United States and has created a funding mechanism
to develop stem cell therapy centers. That's an important
impetus to show it is time for this to be in the clinical arena."
Sonia Skarlatos, acting director of
the National Heart, Lung and Blood Institute's Division of
Cardio-vascular Diseases, is excited by the potential for stem cell–based
therapies in cardiology. Some European studies have shown that infusion
of stem cells from bone marrow has improved left ventricular ejection
fraction, indicating improved pumping ability in damaged hearts.
"It's minimal—just
3% to 4%—but significant and gives us reason to think this
line of research is a positive development in cardiology,"
she says. "Many questions still need to be answered, but there
are certain good signs to be encouraged."
What matters most is that stem cell research
has the potential to revolutionize treatment for heart attack patients
like Carroll Payne. At first, Payne was reluctant to enroll in the
Emory clinical trial because it meant more time in the hospital.
His wife, who happens to be a nurse, quickly convinced him otherwise.
"If there's any possibility
to improve the damage to my heart," says Payne, "it's
well worth it." |
|
| |
|
|
| |
|
|
| |
| |
Getting
to the core of stem cell research |
|
 |
While
Arshed Quyyumi and Edmund Waller are using adult stem cells
to treat heart attack patients, their work will be informed
by the research of anesthesiologist Marie Csete, who directs
the core facility for human embryonic stem cell research
in the School of Medicine.
Csete is working to answer
some still-unknown and critical basic science questions
about stem cells. For instance, how do they age? How does
oxygen mediate the development of embryonic stem cells?
How can they be used to understand drug toxicity in the
developing fetus?
Emory's core facility
does not derive stem cells but maintains stem cell lines
approved for use in federally supported research. The cells
are stored and cultivated in mini-incubators where they
are exposed to low physiologic levels of oxygen of about
3%. This protocol is based on Csete's prior findings
that stem cells exposed to oxygen levels close to those
inside the human body, instead of the oxygen levels found
in a lab's ambient air, are better protected from
chromosomal damage.

The core facility provides
embryonic stem cells to researchers at Emory and those with
the joint Georgia Tech/Emory Center for the Engineering
of Living Tissues. It also serves as a resource center,
providing technical assistance and education for investigators
conducting various stem cell research projects.
Csete collaborates regularly
with researchers outside of Emory, including the University
of Georgia. With UGA, Csete focuses on creating the ideal
gaseous environment to reduce oxidative stress and lower
rates of cell mutation. She also collaborates with the University
of Michigan's Electrical Engineering and Computer
Science Department on a study to develop oxygen gradients
on which stem cells can be grown. The patterning of stem
cells into functional organs takes place along these gradients.
If adult stem cells hold promise
for repairing damaged hearts, why not derive all stem cells
from adults—and avoid the controversy surrounding
the use of embryonic stem cells? According to the NIH, human
embryonic stem cells appear to have significantly greater
developmental potential than adult stem cells. Simply put,
embryonic stem cells may be pluripotent—able to give
rise to cells found in all tissues of the embryo except
for germ cells—as opposed to multipotent adult stem
cells that appear to be restricted to specific subpopulations
of cell types. However, pluripotency comes at a price: Human
embryonic cells are more difficult to control than adult
cells because they have many more options.
Yet, while adult stem cells
are difficult to grow in the lab, embryonic stem cells can
reproduce indefinitely. Because the number of adult stem
cells and their ability to reproduce diminish with age,
obtaining clinically significant numbers of cells can be
difficult.
The issue is not adult versus
embryonic stem cells, however. "Both are important
parts of the big picture," says Waller. "The
embryonic stem cell research that Dr. Csete is conducting
will advance our understanding of how cells work, grow,
and differentiate in ways that ultimately will benefit patients."
To learn more about Csete's
work, visit Momentum magazine's In
the Air and On
Point. |
|
| |
|
|
|
|
| |
|
|
| |
|
|
|
|
|
